Table of contents:
Good Practice: Data Collection
BANGLADESH
Local Authorities Using WISH2ACTION Beneficiary Database to Support Persons with Disabilities[1]
Meetings between the Upazila Social Welfare Officer and the Chairman of Salimpur Union Parishad of Sitakunda Upazila revealed gaps regarding accurate data available for persons with disabilities in the area. To minimize these gaps, Handicap International (HI) provided a list of its beneficiaries to authorities and other relevant stakeholders through the WISH2ACTION project, which the project team prepared with data collected using the Washington Group Questionnaire (WGQ). Local government offices and other stakeholders have since used the database in their initiatives to support persons with disabilities.
Advances in Medical Science and Technology: Gaining Access to Supportive Devices and Technologies
In accordance with the CRPD, State parties are to promote the availability, knowledge and use of supportive devices and technologies designed for persons with disabilities, as they relate to habilitation and rehabilitation.
According to WHO, habilitation and rehabilitation can reduce the impact of a broad range of health conditions (such as diseases and injuries). The World report on disability defines them as sets of measures that assist individuals who experience, or are likely to experience, disability to achieve and maintain optimal functioning in interaction with their environments. Encompassing medical care, therapy and assistive technologies, such measures should begin as early as possible and be made available as close as possible to where people with disability live.
In recent years there have been significant improvements in supportive technologies available for persons with disabilities:
- People with physical disabilities that affect movement can use mobility aids such as wheelchairs, scooters, walkers, canes, crutches, prosthetic devices, and orthotic devices to enhance their mobility.
- Hearing aids can improve hearing ability in persons with hearing impairments.
- Cognitive assistance, including computer or electrical supportive devices, can help people function following brain injury.
- Computer software and hardware, such as voice recognition programmes, screen readers, and screen enlargement applications, help people with mobility and sensory impairments to use computer technology[2].
- In the classroom and elsewhere, supportive devices, such as automatic page- turners, book holders, and adapted pencil grips, allow learners with disabilities to participate in educational activities.
- Closed captioning allows people with hearing impairments to enjoy movies and television programmes.
- Barriers in community buildings, businesses, and workplaces can be removed or modified to improve accessibility. Such modifications include ramps, automatic door openers, grab bars and wider doorways.
- Adaptive switches make it possible for a child with limited motor skills to play with toys and games.
- Many types of devices help people with disabilities perform such tasks as cooking, dressing and grooming. Kitchen implements are available with large, cushioned grips to help people with weaknesses or arthritis in their hands. Medication dispensers with alarms can help people remember to take their medicine on time. People who use wheelchairs for mobility can use extendable reaching devices to reach items on shelves.
- When afforded access to such supportive technologies, persons with disabilities may be better able to live independently and participate in their societies. It has been estimated, however, that in many low-income and middle-income countries only 5 per cent to 15 per cent of people who require assistive devices and technologies have access to them[3].
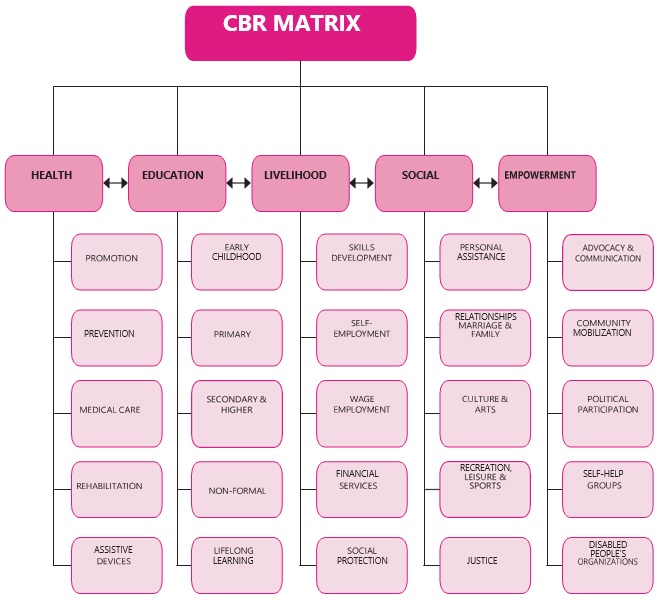
Community-Based Rehabilitation
The CRPD specifies the right of persons with disabilities to live within their communities (Art. 19). Community Based Rehabilitation (CBR) focuses on enhancing the quality of life for people with disabilities and their families; meeting basic needs; and ensuring inclusion and participation. It is a multi-sectoral strategy that empowers persons with disabilities to access and benefit from education, employment, health and social services. It is a strategy within general community development targeted on rehabilitation, equalization of opportunities and social inclusion of all children and adults with disabilities.
CBR is implemented through the combined efforts of persons with disabilities themselves, their families and communities, and the appropriate health, education, vocational and social services[4] . CBR has developed from a medical approach to one based on the human rights of persons with disabilities. Thus, the focus of CBR has evolved from medical rehabilitation towards more comprehensive multi-sector approaches such as access to health care, education, vocational training, income generation programmes and community participation and inclusion. Again, it is essential to have (i) the direct participation of persons with disabilities in planning and implementation of CBR programmes, (ii) increased collaboration between sectors providing services, and (iii) government support in development of national policies. However, as all communities differ in their socio-economic conditions, terrain, cultures and political systems, no single model of CBR is appropriate for all countries or for all parts of an individual country. CBR is an essential component of community development[5].
Key Community-Based Rehabilitation (CBR) Elements for Africa
CBR must:
- adopt a rights-based approach, empowering persons with disabilities and their families;
- involve persons with disabilities, parents and their organizations from the start;
- enable key stakeholders to access information on all issues, including HIV and AIDS;
- look at persons with disabilities holistically;
- advocate for appropriate legislation and policies;
- enhance self-advocacy of disabled persons;
- develop long-term and short-term plans together with all stakeholders, i.e. it must ‘be strategic’;
- ensure inclusion of disability issues in all development programmes, collaborating in all sectors;
- take into consideration local cultures, resources and practices;
- address issues of poverty among persons with disabilities and their families. These elements can also be applied in other countries.
Source: Community-Based Rehabilitation (CBR) as a Participatory Strategy in Africa, Cornell University ILR School, 2002, available at: http://digitalcommons.ilr.cornell.edu/gladnetcollect/60.
Community care and personal social services can be broadly defined as those designed to enable people to remain living in their communities, especially when they have difficulties doing so because of illness, disability or age. The key to ensuring non-discrimination and equal access to health and personal social services is raising the level of awareness of the needs and rights of persons with disabilities. This requires consultation and participation with persons with disabilities at all stages of policy development, programme planning and implementation. Policies and programmes at all levels are consistently better when organizations of persons with disabilities take part in planning from the outset.