Table of contents:
Disability Prevalence Measurements
Disability is an evolving concept and… results from the interaction between persons with impairments and attitudinal and environmental barriers that hinders their full and effective participation in society on an equal basis with others. Preamble, Convention for the Rights of Persons with Disabilities
Measuring the prevalence of disability requires engaging with the questions: what is disability and what does it mean to have a disability? For a long time, research on this topic was dominated by the purely medical model that conceived of disability as the result of a solely physical condition of the individual. Disability measurement was exclusively linked to the diagnosis of medical conditions, their degree of severity and impact on the individual’s ability to work. Consequently, interventions mostly revolved around identifying and treating illnesses to prevent disability and providing medical care and social welfare benefits at the individual level once a disability occurred.
Thanks to advocacy efforts by the disability rights movement, the field has moved away from this clinical approach to a more interactive one that incorporates social and environmental factors.[1] The social-relational approach recognizes that there are barriers in society which turn a person’s impairment into a disability and limit his or her participation. Thus, society must take an active role in removing barriers, such as through legal recognition of the rights of persons with disabilities, provision of inclusive education, workplace accommodation and universal design, meaning that the environment should be designed in a way that makes it accessible to everyone.
Figure 1: ICF model of disability[2]
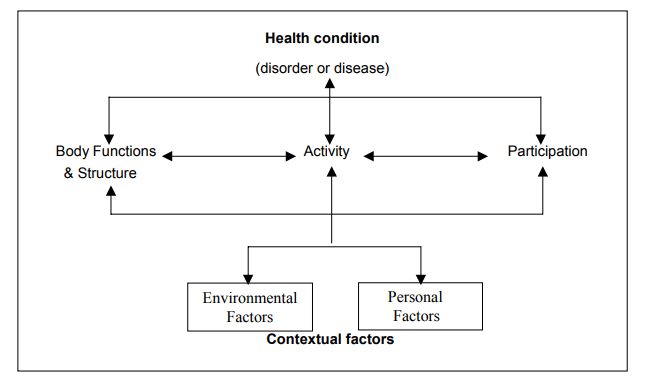
This paradigm shift led to the development of a new framework for health and disability by the World Health Organization (WHO) in 2001: the International Classification of Functioning, Disability and Health (ICF, figure 1). It defines disability as the outcome of interactions between health conditions (disorders or diseases) and contextual factors, both environmental and personal. Disability includes impairments (problems in body function or structure), activity limitations (problems in executing activities) and participation restrictions (problems in involvement in life situations). While the field of disability continues to evolve, with lively debates that reexamine assumptions and approaches, the ICF has become a widely accepted tool that provides the conceptual basis for the definition and measurement of disability at both the individual and population levels.
With growing interest from academia, governments and international development agencies, new measurement tools have been developed to operationalize the ICF. Data collection activities have surged, but they have mostly taken place in more developed countries. The lack of a uniform methodology means that data still are not always comparable over time and across countries.
Recognizing the urgent need for robust, comparable statistics on disability, the United Nations Statistical Commission (UNSC) established the Washington Group on Disability Statistics to produce tested tools for measuring disability. The Washington Group has developed a short set of questions (Washington Group Short Set - WGSS) to capture data on disability in an effective and efficient manner (see box). As of 2017, at least 69 countries have reported using the WGSS or some variant in their most recent censuses, national surveys or disability modules.[3] In countries with reported data, the disability prevalence rate found by using the WGSS is usually above 3 per cent, and often considerably higher (table 1).
The Washington Group Short Set (WGSS) of questions asks about difficulties a person may have doing the most basic activities because of a health problem. These activities are considered universal, occurring frequently and associated with social exclusion.
The six activities are:
- seeing (even if wearing glasses);
- hearing (even if using a hearing aid);
- mobility (walking or climbing steps);
- cognition (remembering or concentrating);
- self-care (such as washing or dressing);
- communicating (understanding or being understood).
For each activity, the respondent is asked to select one out of four levels of difficulty: no difficulty, some difficulty, a lot of difficulty or cannot do at all. The respondent is considered as “having a disability” if he or she answers, “a lot of difficulty” or “cannot do at all” to at least one of the six activities.
Sources: Australian Bureau of Statistics, 2017; Loeb, 2016; Uganda Bureau of Statistics, 2012, p. 28; Statistics South Africa, 2016, p. 33.
| Country | Census/Survey | Year | Rate |
|---|---|---|---|
| Australia | Survey | 2016 | 6.7% |
| Maldives | Survey | 2009 | 9.6% |
| South Africa | Survey | 2016 | 7.7% |
| Turkey | Census | 2011 | 6.9% |
| Uganda | Survey | 2011 | 4.9% |
| United States | Survey | 2012 | 7.9% |
| Zambia | Survey | 2006 | 8.5% |
Countries in the Arab region have adopted this methodology for recent household surveys and censuses. Out of the 14 countries that have provided data to ESCWA, three used the WGSS exactly as intended: Jordan, Morocco and Yemen. Another seven countries used a variant of the WGSS: Egypt, Iraq, Oman, Palestine, Qatar, Saudi Arabia and Tunisia. The countries which used a method other than the WGSS include Bahrain, Mauritania, Sudan and the Syrian Arab Republic. The complete transition to the use of WGSS in all countries will allow for a more in-depth regional and time series analysis.[4]