Table of contents:
Disability Prevalence Rates: A Challenge of Definition and Measurement
Measuring disability prevalence is a complex challenge, especially in developing countries. Results depend to a large extent on the method of data collection as well as on the definition of disability that is applied. Surveys (especially dedicated surveys) often provide more detailed data on persons with disabilities as they allow for the inclusion of more numerous and more in-depth questions. In addition, as they often use nuanced questions and broad definitions of disability that focus on a wide range of limitations and restrictions, such surveys also tend to generate higher and more accurate disability prevalence rates. Population censuses are also commonly used for collecting disability-related data. The advantages of censuses are that they cover entire populations and are conducted at regular intervals, and thus allow for the monitoring of trends over time. However, as censuses only include a limited number of questions on disability and are often based on more narrow interpretations of disability, they tend to produce lower prevalence rates that only reflect a sub-population of persons with more severe impairments.
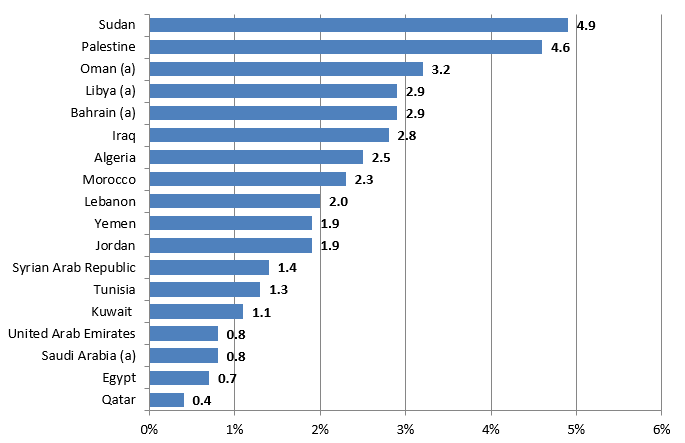
Given the widespread use of censuses for measuring disability in the Arab world, these trends – along with other factors such as the presence of social stigma, which may discourage people from reporting disabilities – may help to explain the remarkably low disability prevalence found in Arab countries. According to available data, disability prevalence ranges from 0.4 per cent in Qatar to 4.9 per cent in the Sudan (see figure 1). Of the 18 countries for which data is available, 15 report disability prevalence under 3 per cent and half report rates under 2 per cent. Such figures contrast sharply with those of other regions as well as with global averages. In Latin America and the Caribbean, for example, average disability prevalence is estimated at 12.4 and 5.4 per cent respectively, whereas the World Health Organization (WHO) and World Bank estimate that approximately 15 per cent of the world population lives with disability. Moreover, disability prevalence in Arab countries is remarkably low given the widespread occurrence of risk factors and disability causes in the region, including consanguinity, communicable and chronic diseases, road traffic accidents and armed conflict.
Figure 1 Disability prevalence in the Arab region (in percentage)
Sources: ESCWA, based on data verified by national statistical offices from the following sources: Algeria: Office National des Statistiques et al. (2006); Bahrain: Central Informatics Organization (2010b); Egypt: Central Agency for Public Mobilization and Statistics (2006); Iraq: Central Organization for Statistics and Information Technology et al. (2007); Jordan: Department of Statistics (2010); Kuwait: Central Statistical Bureau (2011); Lebanon: Central Administration of Statistics et al. (2004); Libya: Pan Arab Project for Family Health and the National Centre for Infectious and Chronic Disease Control (2007); Morocco: Haut-Commissariat au Plan (2004); Oman: National Center for Statistics and Information (2010); Palestine: Palestinian Central Bureau of Statistics (2007); Qatar: Qatar Statistics Authority (2010); Saudi Arabia: Central Department of Statistics and Information (2004); Sudan: Central Bureau of Statistics (2008); Syrian Arab Republic: Central Bureau of Statistics (2007); Tunisia: National Institute of Statistics (2009); United Arab Emirates: National Bureau of Statistics (2005); Yemen: Central Statistical Organization (2004).
Note: a data pertains to nationals only.
Thus, existing disability prevalence rates in Arab countries must be taken with a grain of salt. Reliability and comparability of data across countries is limited not only by the use of varying data collection methods, but also, especially, by the use of different definitions of disability. Even where countries use the same general method of data collection, cross-country comparisons are highly challenging due to a lack of coherence in typologies and classifications of disability. In other words, comparability of data is limited in the Arab region since countries use different categories and terminology to describe different types of disabilities. In order to illustrate this issue, table 1 presents the classifications that a number of Arab countries use to describe disabilities related to mobility and movement-related body structures. The list shows that few countries use the same terminology when collecting data on types of disability, with some countries focusing on people’s impairments (such as ‘paralysis’ or ‘loss of leg’) and others basing their classifications on limitations and difficulties in functioning (such as ‘difficulty in movement’ or ‘difficulty in walking’).
| Bahrain |
|
|---|---|
| Egypt |
|
| Iraq |
|
| Jordan |
|
| Kuwait |
|
| Lebanon |
|
| Libya |
|
| Morocco |
|
| Oman |
|
| Palestine |
|
| Qatar |
|
| Saudi Arabia |
|
| Sudan |
|
| Syrian Arab Republic |
|
| Tunisia |
|
| United Arab Emirates |
|
| Yemen |
|
Sources: Bahrain: Central Informatics Organization (2010b); Egypt: Central Agency for Public Mobilization and Statistics (2006); Iraq: Central Organization for Statistics and Information Technology et al. (2007); Jordan: Department of Statistics (2010); Kuwait: Central Statistical Bureau (2011); Lebanon: Central Administration of Statistics et al. (2004); Libya: Pan Arab Project for Family Health and the National Centre for Infectious and Chronic Disease Control (2007); Morocco: Haut-Commissariat au Plan (2004); Oman: National Center for Statistics and Information (2010); Palestine: Palestinian Central Bureau of Statistics (2007); Qatar: Qatar Statistics Authority (2010); Saudi Arabia: Central Department of Statistics and Information (2004); Sudan: Central Bureau of Statistics (2008); Syrian Arab Republic: Central Bureau of Statistics (2007); Tunisia: National Institute of Statistics (2009); United Arab Emirates: National Bureau of Statistics (2005); Yemen: Central Statistical Organization (2004).
Note: These classifications are taken from the official data sources and thus may not reflect UN terminology.
The International Classification of Functioning, Disability and Health (ICF) represents the central framework for promoting coherent and accurate terminology and classifications related to disability. Developed by WHO, the ICF is a classification system that provides common, standard and comprehensive language to describe health and health-related conditions. Under this framework, disability is understood according to two main components: (i) impairments in body functions (such as seeing and hearing) and in body structures (such as the structure of the eyes and ears); as well as (ii) activity limitations and participation restrictions (such as dressing and eating). Moreover, the ICF defines a set of contextual factors (such as physical geography and societal attitudes), which interact with the above components and serve to impact – positively or negatively – on a person’s functioning and disability/ies. Table 2 provides a list of categories according to the different components of the ICF.
| Body functions |
|
|---|---|
| Body structures |
|
| Activities and participation |
|
| Environmental factors |
|
Source: WHO (2001).